The Sexual and Reproductive Health and Rights of Young People in India a Review of the Situation
Calculation Information technology Up: Investing in the Sexual and Reproductive Health of Adolescents in India
Topic
The time is at present. Volition you stand for reproductive health and rights?
India has made important gains in improving the sexual and reproductive health of women and young people. These advances include the expansion of the contraceptive method mix under the National Family Planning Plan, efforts to strengthen the contraceptive supply chain, and the 2014 launch of the Rashtriya Kishor Swasthya Karyakram (National Adolescent Health Program) , which prioritizes salubrious development during adolescence.i,2
Critical gaps in meeting adolescent sexual and reproductive health needs remain. As a effect of lack of authentic information, provider bias and other barriers, many adolescents have limited bureau to protect and foster their ain sexual and reproductive wellness,iii–five and obtaining comprehensive abortion intendance can be particularly challenging .4,6,vii Difficulties related to obtaining information and services are compounded for adolescents who are marginalized on the footing of their sexuality, gender expression or marital condition.viii–10 Gaps in access to comprehensive sexual and reproductive wellness care must be addressed for all adolescents, so they can exercise their rights to bodily autonomy and pb healthy lives.11–14
The Adding It Up project estimates the need for, touch on of and costs associated with increased investment in essential sexual and reproductive health services, including contraceptive care, maternal and newborn wellness care, and abortion-related intendance. These estimates demonstrate the immense potential benefits of investments to ensure that young women can decide whether and when to accept children and can experience safety pregnancy and delivery. The estimates presented hither pertain to boyish women* anile fifteen–nineteen in Republic of india in 2019.†
Unless otherwise noted, the estimates in this study come from Sully East et al., Calculation It Upwardly: Investing in Sexual and Reproductive Health 2019, New York: Guttmacher Institute, 2020, and its accompanying methodology, which contains sources and methodological details. Some of the key data sources for this report include the United nations (UN) Population Partitioning's World Population Prospects 2019, for population information; the UN Population Partitioning'due south Estimates and Projections of Family Planning Indicators 2020, for unmet demand and current contraceptive use information; the Indian National Family Health Survey (NFHS-iv), for data on subgroup and state-specific service coverage and demand; and the Sample Registration System from the Office of the Registrar General, India, for numbers of maternal deaths. Unless otherwise noted, the data in this report come from calculations based on these sources.
Key points: Agreement the need for and impact and cost of sexual and reproductive health services for adolescent women in Bharat
Need
- two one thousand thousand adolescent women in India have an unmet need for modernistic contraception
- 52% of adolescents giving nativity brand the recommended minimum of four antenatal intendance visits
- 78% of abortions among adolescents are unsafe and thus carry an elevated chance for complications
- 190,000 adolescents do not receive needed intendance following an unsafe abortion
Bear on
If all adolescent women in Bharat wanting to avoid a pregnancy were to apply mod contraceptives and were provided the total spectrum of contraceptive options, counseling and information, and if all needs for maternal, newborn and abortion-related health care were met, annually there would be:
- 732,000 fewer unintended pregnancies
- 482,000 fewer unsafe abortions
Toll
Providing contraceptive care, maternal and newborn health care, and abortion-related intendance to all boyish women in India who need these services would cost ₹11.42 (US$0.16) per capita annually. This includes both the direct costs of providing intendance and the indirect costs associated with programs and systems.
Demand for contraceptive services
In Republic of india, many women get sexually active, marry and start childbearing between the ages of 15 and 19. Many adolescent women—3.4 million—desire to avoid pregnancy. This includes 3.ii one thousand thousand married women and 195,000 sexually agile unmarried women.‡
- Amid adolescent women wanting to avoid a pregnancy, just about i million (29%) are using modern contraceptive methods (Figure 1).

- About one-half (48%) of adolescent women and their partners who use modernistic methods rely on male condoms. 40 percentage use other short-acting methods including 37% who use the oral contraceptive pill and iii% who rely on either injectables, lactational amenorrhea or female condoms. These methods are predominantly obtained from the private sector.fifteen 8 percentage of adolescent women using modernistic methods use permanent female sterilization , and 4% use long-acting reversible methods .
- More than two million adolescent women wanting to avoid a pregnancy (71%) practice not use a modern contraceptive method and are therefore categorized as having an unmet demand for modern contraception. The majority of these adolescents utilise no method at all, while about x% of them apply withdrawal equally their primary form of contraception.
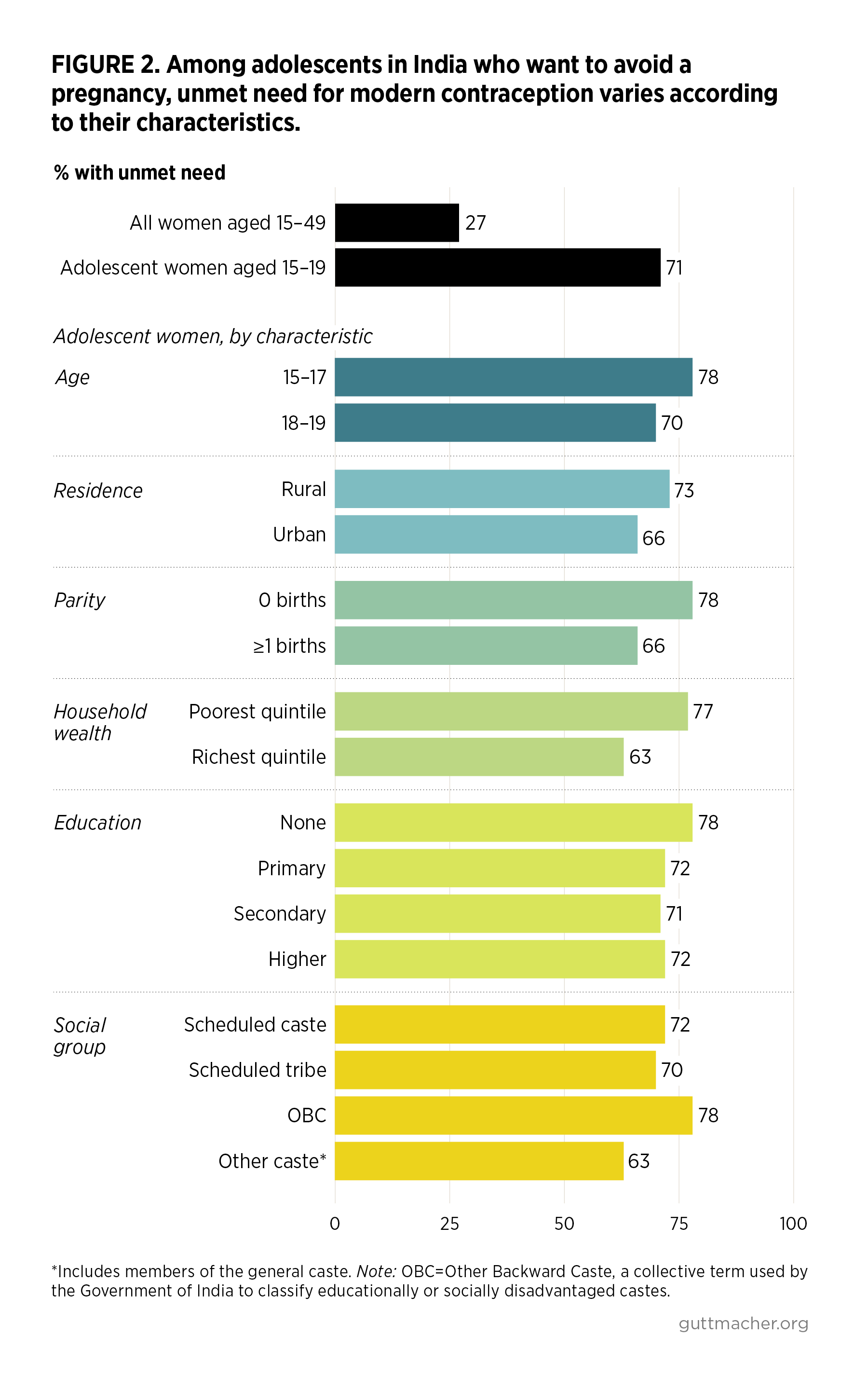
- Amongst women wanting to avoid a pregnancy, the proportion who have an unmet need for modern methods is much higher for adolescents (71%) than for all women in India of reproductive historic period (27%).
- The level of unmet need for modern contraception varies across groups of adolescent women wanting to avoid a pregnancy. For instance, unmet need affects 63% of adolescents from the richest households and 77% of those from the poorest households (Figure 2). Unmet need is also elevated amongst adolescent women in rural areas, those who have not begun childbearing and those younger than xviii.
- Of the 60 million adolescent women in India, two million each yr experience a pregnancy. The bulk of these pregnancies (63%) are unintended, pregnant they occur too before long or are not wanted at all. Adolescent women with an unmet need for modern contraception account for nine out of every ten unintended pregnancies amidst 15–19-twelvemonth-olds.
Need for maternal and newborn health care
Although relatively high proportions of adolescent women giving birth do so in a health facility (85%; Figure 3) and deliver with a skilled nativity attendant (86%), there are still many adolescents whose needs for pregnancy-related health intendance are non existence met, and these gaps vary according to women's characteristics.
- Twoscore-viii percent of adolescent women who experience major medical complications related to pregnancy or delivery do non receive necessary treatment.
- Only 52% of adolescents giving birth receive the recommended minimum of four antenatal care visits.§ This proportion is much lower among adolescents giving nativity who have no education (30%) than among those who accept more than than a secondary didactics (56%), and it is lower amidst rural adolescent women (48%) than among those in urban areas (64%).
- Among adolescents giving birth, the proportion delivering in a wellness facility is lower for women from the poorest households (72%) than for those from the wealthiest households (96%).
- Sixty percent of adolescent women giving birth receive a postnatal checkup within 24 hours of delivery. This proportion is lower amidst rural adolescent women (44%) than amidst married adolescents (60%).
Ballgame-related care
- Of the two million pregnancies that occur among adolescents in India each year, 53% of them end in abortion, resulting in 930,000 abortions annually.**
- An estimated 78% of abortions among adolescents are dangerous (either less safe or least safe). Abortions categorized equally to the lowest degree safe are those most likely to effect in complications.
- Of the 450,000 adolescent women per yr who need postabortion treat complications following an unsafe ballgame, 42% of them (190,000) do non receive it.
- Full provision of both safe abortion care and postabortion care should include counseling on and provision of contraceptives.18
Impact
- Adolescent women who desire to avoid pregnancy need contraceptive services that allow them to make informed choices about their bodies, protect their health and avoid unintended pregnancies, unsafe abortions and maternal death. These services must include nonjudgmental contraceptive counseling, provision of the full spectrum of contraceptive options, and full information about right method utilise, potential side effects and management of side effects.
- If all adolescent women in India who want to avoid a pregnancy were using modern contraceptives and all significant adolescents were to receive care at the standards recommended by the World Health Organization (WHO), the impacts would be dramatic: Unintended pregnancies and unsafe abortions would decline past 66% (Table one).
- Further, if all abortions that are currently unsafe were provided safely, and if all needs for contraceptive and postabortion care were met, abortion-related deaths would decline by 97%.

Costs
- The annual combined cost of providing current levels of contraceptive, maternal, newborn and abortion-related intendance for adolescent women in India is estimated at ₹1,073 crore, or US$147 million†† (Effigy 4).

- This full includes ₹67 crore (United states$9 meg) for contraceptive services, ₹654 crore (The states$89 one thousand thousand) for maternal and newborn health care, and ₹353 crore (U.s.$48 million) for abortion-related care. Annual direct costs‡‡ are ₹553 crore (US$75 meg) and annual programs and systems (indirect) costs are ₹521 crore (US$71 million).
- A comprehensive packet of sexual and reproductive health care that would run into all adolescent women'south needs for modern contraceptive services (including contraceptive counseling), maternal and newborn health intendance, and ballgame-related intendance, would cost ₹1,561 crore (The states$213 million) annually.
- This comprehensive package would really toll less than increased investment in maternal and newborn health care lone. Because investing in contraception averts unintended pregnancies, every boosted ₹100 spent on contraceptive services to a higher place the current level would save ₹252 (or U.s.a.$2.52 saved for every The states$1 spent) in the cost of maternal, newborn and abortion-related intendance.
- In improver, providing total admission to comprehensive safe ballgame intendance would reduce the incidence of abortion-related complications and, therefore, the cost of postabortion care. The overall costs associated with abortion-related care would decrease by ₹297 crore (U.s.$41 one thousand thousand) to ₹56 crore (US$8 one thousand thousand) annually.
- In improver to immediate price savings and improvements in health, increased investment in sexual and reproductive health would also attain far-reaching long-term benefits to households and society at large. For example, the Population Foundation of India estimated that 15 years' worth of appropriate public investment in modernistic contraceptive care could salvage households 1-fifth of their out-of-pocket expenditures on kid health care costs, and cause Bharat'due south per capita gross domestic product to rising by 13%.19
Recommendations
Targeted investment in the sexual and reproductive health of adolescents in India is vital to reducing unintended pregnancies, unsafe abortions, unplanned births and maternal deaths, as well as to ensuring the actual autonomy and well-being of the state's young people. In addition to total investment, a rights-based policy framework is needed to prevent reproductive coercion and ensure equity in access to services. The following shifts in policies, programs and practices will be required in society to meet health goals set at country and global levels.
Help adolescents make informed decisions by providing them with high-quality, inclusive, accessible and nonjudgmental contraceptive counseling services.
- Health workers must provide adolescents with accurate, nonbiased information.
- All health workers must be trained in how to provide adolescent-friendly services, including how to provide respectful, nonjudgmental care for young people, regardless of their marital status or gender. Value clarification exercises that betrayal underlying judgments and behavior around boyish sexual health may help health workers provide adolescents with the same quality of care they offer older women.
- Information on contraception needs to be provided to single boyish women and men through multiple channels, and then that their first betoken of contact with the wellness arrangement is not for maternity intendance.
- Contraceptive counseling for adolescents must include information about a range of contraceptive methods, every bit well as each method's effectiveness, potential side effects and cost; assistance in choosing a method that matches their childbearing goals (including information about the utilize of temporary methods for preventing, delaying or spacing births); STI prevention strategies; and information on emergency contraception and abortion services for adolescents whose chief method has failed.
Diversify efforts to disseminate information and provide sexual and reproductive health care.
- Private-sector channels must be strengthened to ensure high-quality and comprehensive care, particularly for contraceptive services focused on spacing births, equally adolescents tend to seek this care from providers outside of the public sector.15
- Social marketing and digital solutions, including social media campaigns, must exist leveraged to reach young people unable to obtain care through traditional channels.
- Adolescent women must be provided with data, commodities and support according to WHO guidance for self-care in sexual and reproductive health. Sexual and reproductive wellness services must reach adolescents who desire to self-administer methods of contraception, such every bit oral contraceptives and injectables, as well as medication abortion.
Strengthen national laws and policies to protect the rights of adolescents to sexual and reproductive health care.
- Comprehensive, stigma-free contraceptive and abortion services must be accessible for all adolescents.
- Age-appropriate comprehensive sexuality didactics that affirms young people's rights, including their correct to pleasure, must be offered through community- and schoolhouse-based programs. These programs should provide data on fertility awareness, pregnancy and contraceptive options.
- Government family planning programs, such as Mission Parivaar Vikaas, should broaden their language so that messages nigh preventing unintended pregnancy employ to all people, regardless of their marital status.
- The high rates of child marriage establish in some states must be addressed through increased education about the harmful social norms and practices that perpetuate early on matrimony, and by enforcing the legal historic period of marriage. This blazon of multipronged arroyo is necessary to ensure girls' physical safety and reproductive autonomy.
- Young people must be meaningfully engaged in conceptualizing, designing, implementing, monitoring and evaluating programs and policies that affect them, in accordance with guidance from WHO's Global Accelerated Action for the Wellness of Adolescents (AA-HA!).
Lastly, adolescent sexual and reproductive health must be prioritized amidst the spread of COVID-nineteen to avoid disruption of awareness efforts and service commitment, which could widen existing gaps in health outcomes and access to care.
Footnotes
*We use the term "women" to match the data available in the National Family Wellness Survey (NFHS-4), although nosotros recognize that non all people needing and using contraceptive, maternal, newborn or abortion-related care identify as women.
†Estimates for all women aged 15–49 in Republic of india can be plant in Guttmacher Found, Adding It Upward: investing in the sexual and reproductive wellness of women in India, Fact Sheet, New York: Guttmacher Institute, 2020.
‡We assume all married women are sexually active and define unmarried women as sexually agile if they had sex in the xxx days prior to the survey. Adolescents reporting current contraceptive utilise, regardless of how recently they have been sexually active, are classified every bit wanting to avoid a pregnancy.
§In 2016, the World Health Organization updated its minimum recommended level of care from four antenatal visits to eight contacts with the health system during pregnancy, including through customs outreach;16 however, bachelor data from the National Family Health Surveys are not sufficiently detailed to measure this updated standard of intendance.
**Abortion rates amidst adolescents are estimated using subregional age-specific data, and abortion safety is estimated using data from all women of reproductive age in India. This report uses the revised 2017 WHO definition of ballgame rubber.17 Rubber abortions are those that use a WHO-recommended method advisable to the pregnancy duration and are done by a trained provider. Less-safe abortions meet simply i of these criteria, and to the lowest degree-safe abortions see neither benchmark. We apply "dangerous abortion" to refer to the sum of less-safety and least-rubber abortions.
††As of Feb 2021, in that location were 73.19 rupees per U.S. dollar.
‡‡The sum of personnel time (including provision of information and counseling), contraceptive commodities, medications, diagnostic tests, consumable supplies and food costs during hospital stays. Most of the sources we utilize to gauge direct costs for contraceptive bolt, drugs and supplies reflect public-sector prices and may therefore underestimate actual costs.
References
1. Centre for Health Informatics, Ministry of Health and Family Welfare, Rashtriya Kishor Swasthya Karyakram (RKSK), 2015, https://www.nhp.gov.in/rashtriya-kishor-swasthya-karyakram-rksk_pg.
2. Heart for Health Computer science, Ministry building of Health and Family Welfare, National Program for Family unit Planning, 2018, https://www.nhp.gov.in/national-programme-for-family unit-planning_pg.
3. Jejeebhoy SJ, Sexual and reproductive wellness among youth in Bihar and Jharkhand: an overview, Economic and Political Weekly, 2007, 42(48):35–39.
4. Ganatra B and Hirve S, Induced abortions among adolescent women in rural Maharashtra, India, Reproductive Health Matters, 2002, 10(19):76–85, doi:10.1016/S0968-8080(02)00016-two.
5. Santhya KG and Jejeebhoy SJ, Sexual and reproductive health needs of married adolescent girls, Economic and Political Weekly, 2003, 38(41):4370–4377.
half dozen. Ganatra B, Immature and vulnerable: the reality of unsafe abortion amid adolescent and young women, ARROWs for Change: Women's, Gender and Rights Perspectives in Health Policies and Programmes, 2006, 12(6):1–2.
vii. Jain D and Tronic B, Conflicting abortion laws in Bharat: unintended barriers to safe abortion for boyish girls, Indian Journal of Medical Ethics, 2019, IV(4):310–317, doi:10.20529/IJME.2019.059.
8. Rose-Clarke 1000 et al., Adolescent girls' health, diet and wellbeing in rural eastern India: a descriptive, cross-exclusive community-based study, BMC Public Health, 2019, 19(1):673, doi:10.1186/s12889-019-7053-1.
ix. Sebastian MP, Khan ME and Sebastian D, Unintended pregnancy and abortion in India: country contour report, Footstep Upward Enquiry Report, New Delhi: Population Council, 2014.
ten. Muttreja P and Singh S, Family planning in India: the way forward, Indian Periodical of Medical Research, 2018, 148(Suppl. 1):S1–S9, doi:10.4103/ijmr.IJMR_2067_17.
11. Kumari Due south et al., Teenage marriages and induced abortion among women of reproductive historic period group (15–49 years) residing in an urbanized village of Delhi, Indian Journal of Youth and Adolescent Health, 2019, six(1):xv–xx, http://medical.advancedresearchpublications.com/index.php/IndianJ-Youtha....
12. Basavaraj S and Chakraverty I, Comprehensive sexuality education: the way forwards, Country Advocacy Brief: India, New Delhi: YP Foundation and Pravah, 2017, https://arrow.org.my/wp-content/uploads/2017/x/Republic of india-CSE-brief.pdf.
xiii. Barua A, Waghmare R and Venkiteswaran S, Implementing reproductive and child health services in rural Maharashtra, India: a pragmatic arroyo, Reproductive Health Matters, 2003, 11(21):140–149, doi:10.1016/S0968-8080(03)02162-1.
14. Tripathi N and Sekher Boob tube, Youth in India fix for sex educational activity? Emerging evidence from national surveys, PLOS One, 2013, 8(8):e71584, doi:ten.1371/periodical.pone.0071584.
15. Reproductive Health Supplies Coalition, Article Gap Analysis 2019, 2019, https://www.rhsupplies.org/cga/cga_2019_print_version_final.pdf.
16. World Health System (WHO), WHO Recommendations on Antenatal Care for a Positive Pregnancy Feel, 2016, http://apps.who.int/iris/bitstream/handle/10665/250796/9789241549912-eng....
17. Ganatra B et al., Global, regional, and subregional classification of abortions by rubber, 2010–xiv: estimates from a Bayesian hierarchical model, Lancet, 2017, 390(10110):2372–2381, doi:x.1016/S0140-6736(17)31794-four.
xviii. WHO, Wellness Worker Roles in Providing Rubber Abortion Care and Mail-Ballgame Contraception, 2015, http://world wide web.who.int/reproductivehealth/publications/unsafe_abortion/abort....
19. Population Foundation of India, Cost of Inaction in Family Planning in India: An Assay of Health and Economic Implications, 2018, http://www.indiaenvironmentportal.org.in/files/file/Cost%20of%20Inaction....
Suggested Citation
Murro R et al., Adding It Up: Investing in the Sexual and Reproductive Wellness of Boyish Women in India, New York: Guttmacher Institute, 2021, https://www.guttmacher.org/report/calculation-it-up-investing-in-sexual-repro....
DOI: https://doi.org/10.1363/2021.32662
Acknowledgments
This report was written by Rachel Murro and Elizabeth A. Sully, both of the Guttmacher Institute, and Rhea Chawla, Souvik Pyne and Shruti Venkatesh, all of The YP Foundation. It was edited by Haley Brawl, and figures and tables were designed past Louis Guzik and Michael Moran, all of the Guttmacher Institute.
The authors thank the following reviewers: Subha Sri Balakrishnan, CommonHealth; William Joe, Establish of Economic Growth; Shveta Kalyanwala, independent consultant; and Ajay Kumar Khera, EngenderHealth.
This report was made possible past a grant from the Pecker & Melinda Gates Foundation. The findings and conclusions contained within are those of the authors and do not necessarily reflect the positions or policies of the donor.
Source: https://www.guttmacher.org/report/adding-it-up-investing-in-sexual-reproductive-health-adolescents-india
0 Response to "The Sexual and Reproductive Health and Rights of Young People in India a Review of the Situation"
Post a Comment